Guide: Submitting a Case to Medi-Cal Online
These days, Medi-Cal strongly prefers that you submit your cases online. Sometimes if you send a physical form, it just won’t get processed.
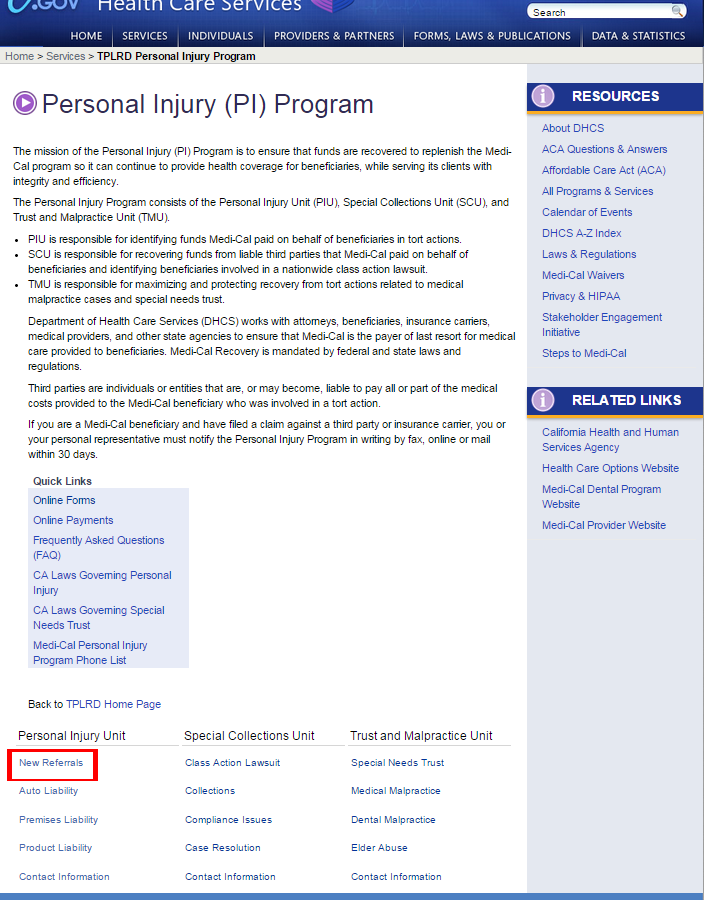
Step 1: Go to the Medi-Cal Website.
Step 2: Click “New Referrals”
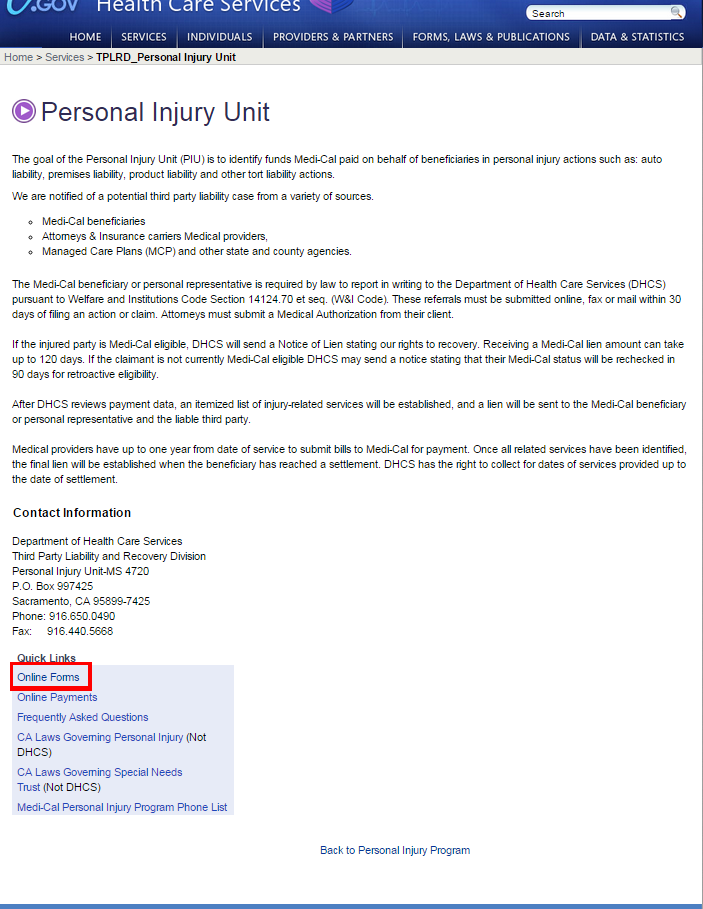
Step 3: Click “Online Forms”
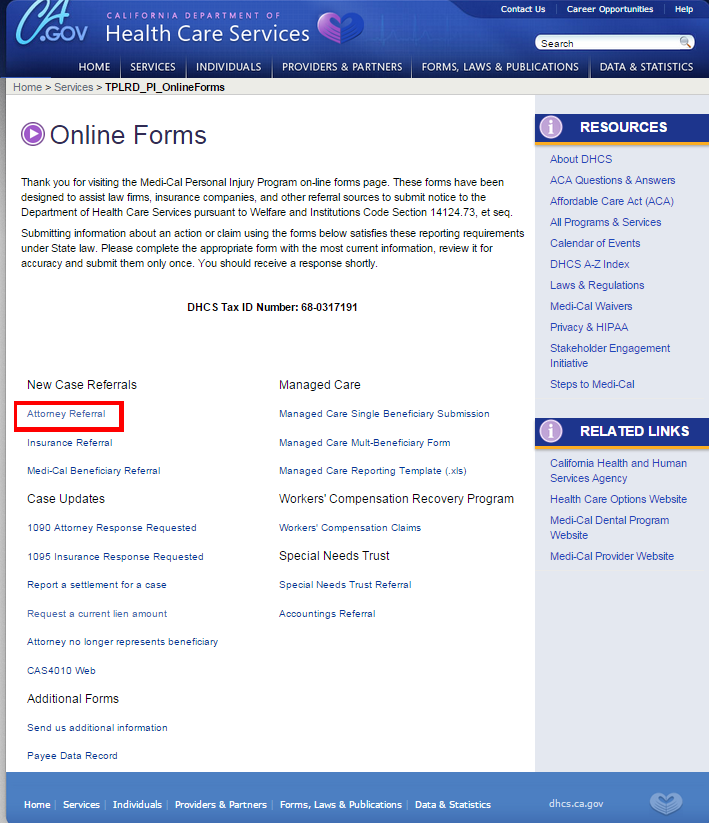
Step 4: Click “Attorney Referral” (or other type if you are not an attorney)
Step 5: Fill Out the Online Form
The Medi-Cal website will “time out” after 15 minutes, so you should have the following information available to copy and paste. Note: You should have a PDF of the Complaint ready to attach to the form.
Part 1 | Who Are You?
First and Last Name:
Phone Number
Email Address:
What is the attorney’s first and last name?
What is the law firm’s name?
What is the attorney’s address?
What is the attorney’s phone number?
Ext:
Does the attorney represent the plaintiff or defense?
PlaintiffDefense
Part 2 | Injured Beneficiary
Beneficiary first and last name:
Beneficiary date of birth:
Please provide the beneficiary’s Medi-Cal Number (MCN) to help identify the injured party.
Medi-Cal Number:
If you are the defense counsel, is this bene acting pro per?
Part 3 | About the Injury
What is the date of injury?
What is the type of injury?
If this was an auto accident, is Medical Payment available?
YesNoN/AIf you stated “Other”, please describe
Describe injury and treatment provided to date:
Was the beneficiary transported in an ambulance?
YesNoUnknownWho caused the injury? (If name is unknown, enter “unknown”)
Part 4 | Injury Causer’s Insurance
What is the policy holder’s name?
What is the insurance company’s name?
What is the insurance company’s address?
What is the claim adjuster’s name?
What is the claim adjuster’s phone number?
What is the policy number?
What is the claim number?
Part 5 | Beneficiary’s Auto Insurance
If the beneficiary was not in an auto accident, please skip to part 6.
If “Yes”, what was the Medical Payment Amount?
How much was used to pay medical providers?
What is the policy holder’s name?
What is the insurance company’s name?
What is the insurance company’s address?
What is the claim adjuster’s name?
What is the claim adjuster’s phone number?
What is the policy number?
What is the claim number?
Part 6 | Opposing Counsel Information
What is the attorney’s name?
What is the firm’s name?
What is the attorney’s address?
What is the attorney’s phone number?
Part 7 | Other Information
If an action has been filed in court, please provide the following
What is the civil complaint number?
What county was the complaint filed in?
Please provide a PDF copy of the filed complaint (Attachments shall not exceed 2MB combined)
FileUpload
Comments:
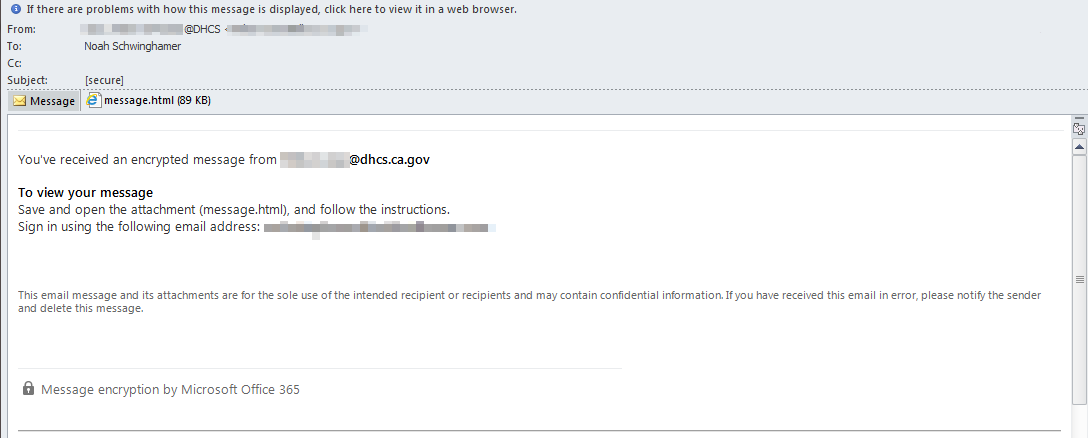
Step 6: (Possibly) Respond via E-mail
DHCS e-mails look a lot like spam, but they are real. This is an example of a real e-mail below. You may wish to add the address “@dhcs.ca.gov” to your trusted e-mail list.